- Fact Sheet: The Biden-Harris Administration Highlights Investments in Rural America, Invites Public Nominations for Rural Innovators Initiative
- Rural Victims of Intimate-Partner Violence Need More Resources and Support, Study Finds
- A Tribe in Maine Is Using Opioid Settlement Funds on a Sweat Lodge to Treat Addiction
- Fact Sheet: USDA, HHS Announce New Actions to Reduce Impact and Spread of H5N1
- Call for Experts: Forum on Aging, Disability, and Independence
- Bill to Expand Definition of 'Village' Qualifying for Water Funds Passes Alaska House
- Child Care Workers Caught in Middle of Michigan's Broken Child Care System
- Few Options Available for Substance Abuse Treatment in the Big Bend
- In Rural Texas, ERs Are Facing a Growing Mental Health Crisis
- Ways and Means Members Put Forth Solutions to Strengthen Telehealth Access and Improve Health Care for Rural Communities
- Sage Memorial Hospital in Navajo Nation Constructs New Facility to Improve Health Care
- How the State, Tribes and Federal Government Are Working to Curb SD's Syphilis Epidemic
- Rural Children Struggle to Access Hospital Services, Say Researchers
- RPHARM Program Fulfills Need for Rural Pharmacists
- A Pilot Program in Rural Vermont Hopes to Build a Blueprint for Substance Abuse Recovery
Medicare Outpatient Payment Policies Finalized
On November 1, CMS finalized updates to the Medicare Outpatient Prospective Payment System (OPPS) and Ambulatory Surgical Care Center (ASC) Payment System for the 2020 calendar year. In addition to updating payment rates, this rule finalizes completing the two-year phase-in of site neutral payment for clinic visits when provided at an off-campus provider-based department. This final rule also finalizes to pay Average Sale Price (ASP) minus 22.5 percent for 340B-acquired drugs for CY 2020. Rural sole community hospitals are still exempted from the reduction and will continue to be paid ASP plus 6 percent. In the rule, CMS finalizes a change to the generally applicable minimum required level of supervision for hospital outpatient therapeutic services furnished by all hospitals and Critical Access Hospitals (CAHs) from direct supervision to general supervision. CMS is also finalizing for the OPPS, the other wage index policies adopted in the FY 2020 IPPS final rule. CMS plans to finalize these provisions on price transparency and requirements for making public a list of standard charges in a standalone document at a later date. As part of this rulemaking, CMS is accepting comments on the payment classifications assigned to the interim APC assignments and/or status indicators of new or replacement Level II HCPCS codes until 5 pm EST on December 2, 2019. Click here for more information from the Federal Register.
CMS Finalizes Medicare Clinician Policy, Payment, and Quality Provisions for CY 2020
On November 1, CMS issued a final rule that includes updates to payment policies, payment rates, and quality provisions for services furnished under the Medicare Physician Fee Schedule (PFS) effective on or after January 1, 2020. This includes three new telehealth codes to describe a bundled episode of care for treatment of opioid use disorders, Medicare coverage for opioid treatment programs, updates to care management services, implementation of a ground ambulance data collection system, and a revision to the current supervision requirement to clarify physician supervision requirements for physician assistants (PAs), among other updates. The rule also makes updates to Medicare’s Quality Payment Program including performance thresholds and category weights for the 2020 performance period and clarifying the definition of rural for the purposes of the Merit-Based Incentive Payment System (MIPS). As part of this rulemaking, CMS included an interim final rule with comment period (IFC) to establish coding and payment for evaluation and management, observation and the provision of self-administered Esketamine, with comments on that proposal due no later than 5 pm on December 31, 2019. Click here for more information from the Federal Register.
Deadline for Critical Access Hospitals to Submit a Hardship Exception Application – December 2
CMS requires that all Critical Access Hospitals (CAHs) use either the 2014 or 2015 Edition certified electronic health record technology (CEHRT) to meet the reporting requirements of the Medicare Promoting Interoperability Program and successfully demonstrate meaningful use. Downward payment adjustments must be applied to CAHs that are not meaningful users of CEHRT. However, CAHs may avoid the Medicare downward payment adjustments by completing a hardship exception application by December 2 to show that meeting the meaningful EHR user requirements would result in a significant hardship. Click here for more information.
AJPH Call for Papers on Rural Public Health –
The American Journal of Public Health (AJPH) invites papers assessing the role of government policy in the status and revitalization of rural health. They seek papers that describe rural health research, report on interventions in rural settings, assess the impact of laws and policies, and examine the human health impact of climate change in rural areas. AJPH also invites editorials and commentaries proposing ways to apply public health methods that have been successful in other regions of the world, describing potential sources of funding, and depicting a vision for a rural public health of the 21st century. Potential authors should visit the AJPH website to review instructions for authors and specific guidelines for the various types of manuscript formats. Abstracts are due on January 15, 2020.
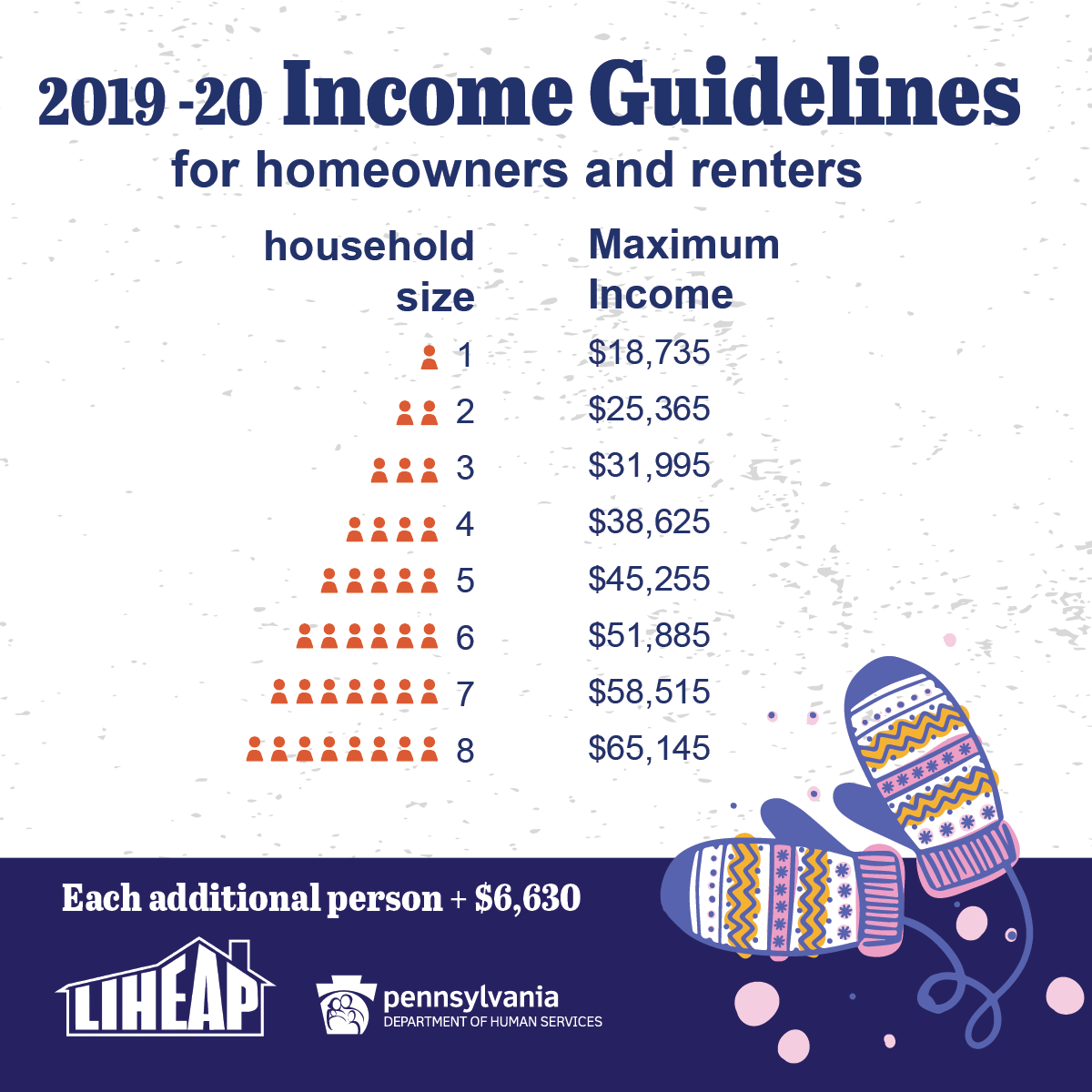
Home Heating Assistance is Now Available for Pennsylvania Families
LIHEAP, which stands for the Low-Income Home Energy Assistance Program, helps families living on low incomes pay their heating bills in the form of a cash grant. Crisis grants also are available for households in immediate danger of being without heat.
How cash grants work
A one-time payment is sent directly to the utility company/fuel provider and is credited on the heating bill. Cash grants range from $200 to $1,000 based on household size, income, heating region, and fuel type.
Qualifying crisis situations
- Broken heating equipment or leaking lines that must be fixed or replaced
- Lack of fuel
- Main heating source has been completely shut off
 Danger of being without fuel (less than 15-day supply)
Danger of being without fuel (less than 15-day supply) - Danger of having utility service terminated (received a notice that service will be shut off within the next 60 days)
Eligibility
- There are income guidelines.
- Applicants do not have to be on public assistance.
- Applicants don’t need to have an unpaid heating bill.
- Applicants can rent or own their home.
What’s needed to apply?
- Names of people in the household
- Dates of birth for all household members
- Social Security numbers for all household members
- Proof of income for all household members
- Recent heating bill or delivery receipt from the previous year
[For crisis situations, a person may need a copy of the shut-off notice.]
How to apply
Pennsylvanians can apply for LIHEAP three ways: online, on paper, and in person.
Online
Apply for LIHEAP benefits online using COMPASS. New this year: Those who received LIHEAP last year can apply for home-heating assistance via the mobile app, myCOMPASS PA. They’ll need the preseason application or green postcard we sent via mail to apply on the app.
On paper
Pennsylvanians can download an English or Spanish version of the application, fill it out, and return it to their county assistance office.
In person
Pennsylvanians can visit their county assistance office for help filling out the application in person. Applications also are available at senior centers and other community agencies.
Contact us for help
For more information about LIHEAP, Pennsylvanians can call the LIHEAP hotline at 1-866-857-7095, or can contact their county assistance office, Monday through Friday. Individuals with hearing impairments may call 711.
Visit the website
Find all of this information and more on the DHS website. View the state plan for LIHEAP and download brochures to print and share.
Forbes Explains How Urbanization Exacerbates the Health Care Crises in Rural America
Forbes reports that according to the USDA’s Economic Research Service, between 2010 and 2017, almost 1,000 rural counties in the U.S. recorded more deaths than births. Simultaneously, rural populations have declined, with only 20% of the population residing in rural areas which make up 97% of the country. Population change also means significant changes in health care need, demand and access. Also, according to the National Institute for Health Care Management (NIHCM), “As urbanization increases, an older, sicker and poorer population remains in rural America.” What this means is that Americans living in rural areas of the country have much greater health issues, and far fewer health resources.
Support for the Rural ACO Improvement Act Builds
The Rural ACO Improvement Act (S.2648) is gaining momentum on Capitol Hill. The recently introduced Senate bill would revise the Medicare Shared Savings Program benchmarking process and level the playing field for rural accountable care organizations. NRHA supports and applauds the legislation as a critical step to ensure all providers, regardless of zip code, are able to benefit from the program. We are proud that other associations with vested interested in the future of rural health care, such as AAFP, are joining us in supporting this meaningful rural health legislation.
Several Hospital Associations in Rural States Support a Senate Finance Rural Health Package
Rural hospital leaders nationwide are urging lawmakers to respond to the rural health care crisis. As rural hospitals are left with tough choices, like shutting down their obstetric unit, policy changes are necessary. New reporting claims that several state hospital associations are in support Congress enacting legislative fixes to ensure the sustainability of rural hospitals. The various state hospital associations support a rural health package with NRHA-backed solutions, such as allowing struggling rural PPS hospitals to convert to CAHs, and a long-term solution of a new payment model. We look forward to working alongside these associations as we urge Congress to act.
NRHA Appropriations Watch Update
During the week of October 28, 2019, the Senate appropriators passed their four-bill minibus focused on domestic spending, yet they have not start debating the second minibus, which contains the L-HHS spending measures. According to Politico, the debate was postponed by Senate Democrats who believe that the 302(b) allocation for the L-HHS bill is too low. NRHA would also like to see more robust funding, particularly for rural health priorities, in the Senate’s version of the L-HHS bill, but we understand that as the appropriations process is postponed, another Continuing Resolution is likely to be employed to ‘buy’ time. However, there is support from congressional leaders and the White House to have the appropriations bills finalized before the end of the year. So, even with the impeachment inquiry underway, we remain optimistic that progress will be made on passing/finalizing federal funding measures.
Health Care Provider Deserts May Leave Patients in the Cold
Rural Affordable Care Act insurance consumers may need to travel farther for care

People with ACA health insurance may be more likely to find themselves in “artificial provider deserts,” according to new Penn State research.Image: GettyImages Adventure_Photo
UNIVERSITY PARK, Pa. — People with health insurance under the Affordable Care Act (ACA) may have access to fewer health care providers — and may also have to drive further to see them — than people with other plans, according to researchers.
In a new study — published Nov. 4 as part of the November issue of Health Affairs — researchers found that people with ACA health insurance are more likely to find themselves in “artificial provider deserts,” areas where the health care providers near a customer are not covered by their insurance plan, leaving them without access to care even though providers are nearby.
Simon Haeder, assistant professor of public policy, said this is usually not a problem for people living in cities, but it can quickly become an issue for people living in more rural areas.
“If you’re of high socioeconomic status and relatively healthy, traveling long distances for care might be easier or not be a big issue for you,” Haeder said. “But if you’re more economically disadvantaged, and if you potentially don’t speak English or have multiple medical conditions, these challenges with provider networks can have large implications for your health.”
The researchers said that after the ACA was passed, there was a lot of research done on how ACA plans compared to commercial plans, like the ones people access through their employers. Haeder said that while this previous work found that ACA plans covered fewer providers and had lower premiums, researchers did not factor in how far people had to travel to see the health care providers covered by their insurance.
Read the entire press release here.